Depression is the most common psychiatric disorder in the elderly population, 10-25% of people over 65 years suffer from significant depressive symptoms.
Depression, is frequently co-morbid with medical illnesses, has a negative impact on the quality of life, increases the number of visits to different medical services, and carries a high risk of suicide, especially in men. Despite these factors, depression in the elderly is under-recognized, particularly in primary care practices, general hospitals, and nursing homes.
The etiology of depression in the elderly is clearly multifactorial and several important contributory risk factors have been identified, including normal aging process, medical illnesses, chronic painful conditions, deficiency of essential nutrients, drug therapy, and psychosocial influences such as retirement, dependency, elderly neglect, death of spouse etc.
Elderly depression is different from depression of young and middle aged patients;
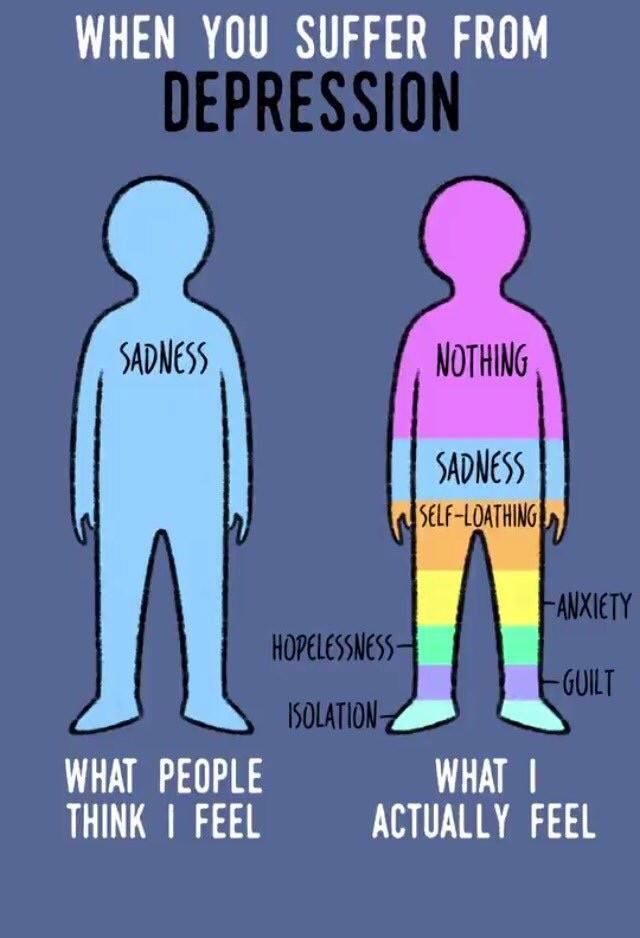
The following are certain symptoms of depression most commonly found in elderly.
- Agitation, anxiety
- Persistent, vague or unexplained physical complaints
- Memory problems; difficulty concentrating
- Social withdrawal, feelings of discouragement or hopelessness, inappropriate guilt
- Lack of attention to personal care
- Irritability and demanding behavior
- Prolonged grief after a loss
- Erratic sleep and appetite patterns.
- Suicidal thoughts or attempts.
- Depression may be early symptom of impending dementia & Parkinsonism.