















Schizophrenia
One in seven Indians is affected by mental disorders of varying severity. The relative contribution of mental disorders to the total disease burden in India has almost doubled since 1990. particularly schizophrenia.
Schizophrenia is a prolonged and major psychiatric disorder that affects how a person thinks, feels, and behaves and severely impairing the individual’s quality of life and their prospects for employment, marriage and parenthood. People with schizophrenia may seem like they have lost a sense of reality.
Symptoms
Schizophrenia is a type of mental illness characterized by distortions in thinking, perception, emotions, language, sense of self and behaviour. Common experiences include:
The five cardinal features of the disorders are:
- Delusions
- Hallucinations
- Disorganized speech
- Disorganized behaviour
- Negative symptoms

Delusions
A delusion is a belief held by the patient, which is false and held firmly by him/her despite its contrary and not shared by their family members or society.
- Delusion of persecution: A person believed that his food was poisoned by his family members and refused to eat, despite repeated reassurance.
- Delusion of jealously( infidelity): A chronic alcoholic believed that his wife was unfaithful and used to harm her even though all his relatives explained that it was false.
- Delusion of reference: A 30-year-old lady believed that all her neighbourhood men and women talked ill of her and repeatedly quarrel with them.
- Delusion of disease (somatic delusion): A 70-year-old male person believed that he has stomach cancer and had gone to various physicians and surgeons for its treatment, even though all examinations and investigations were proved negative.
5. Delusion of guilt or sin: A 40year old lady believed that she deserves punishment by death as she had missed going to the temple last weekend.
6. Bizarre (scientifically not possible) delusions: The 17-year-old student believed that cosmic rays are sent by a satellite from Jupiter, and that is controlling all his actions, including his speech and his movement. B. A 25year old telephone operator believed that all the people in the city knew all his thoughts through telephone lines as a transmitter is fixed in his brain.
7. Delusion of grandeur: A 25year old farmer believed that he was a landlord and owned thousands of acres of land, even though he was a coolie in others field.
The above examples have few things in common
-They are all false belief, believed by the patient only.
-They persist firmly despite giving the proof that it is wrong.
-The belief is not shared by other members of his/her family or his neighbours.

Hallucinations
These are abnormal sensations felt by the patient himself without any external stimulus.
For example, he can see things where others cannot see or hear voices where others couldn’t hear.
Types of hallucinations
Visual hallucinations: here, the patient can see things (humans, animals, or other objects) where others cannot.
Auditory hallucinations: patients could here noise or even voices that others couldn’t.
Auditory hallucinations are most common in schizophrenia; patients hear them, the voices may be threatening or abusive, and some times it may be commenting on the patient’s actions. In some instances, patients report that they could hear their own thoughts aloud. Patients are usually perplexed and maybe found answering to these voices (thus, we may see them talking alone).
Tactile hallucinations: patients could feel sensations over or under their skin like insects crawling even though there are no visible insects around.
Others of smell (olfactory hallucinations) and taste (gustatory hallucinations) which are usually rare to find.


What does a hallucinating patient do?
Usually, patients who are experiencing such hallucinations believe that they are real and do act upon them.
For example, a patient hearing a voice that falls into the well may commit suicide by doing so, or a patient experiencing tactile sensations of insects crawling would clean himself repeatedly.
Disorganized behaviour
Any behaviour that is out of routine and found abnormal to his culture is known as disorganized.
For example: not bathing, not brushing teeth, filthy clothes, collecting waste or garbage or behaving abnormally like urinating in public or doing abnormal body movements.


Disorganized speech
– Patient’s speech is abnormal, which is challenging to understand as it is out of the track, and the sentences are in no connections with each other.
Loosening of associations is an everyday speech disorder where the sentences are not in continuity with each other, and it isn’t easy to understand to the listener.
For example, a patient with schizophrenia commented about the Indo Pak cricket match;
“Indian cricket team came to Pakistan played with Pakistan draw the match eat the chicken sees the Tajmahal rose is beautiful Vajpayee is prime minister football is boring”.
Negative symptoms (the five A’s)
These are the characters of the patients which is deteriorated after the onset of the disease,
- Apathy or avolition-poor grooming and hygiene, physical anergia(appear lazy), irregular to work or school
- Affective flattening-reduced emotional responses, poor eye contact while conversing, decreased spontaneous movements and often inappropriate affect.
- Alogia-poverty of speech, poverty of content and increased response latency.
- Anhedonia or asociality-reduced interest in recreation, being with people or enjoying life
- Attention-poor while testing or while speaking with people.
He may even sit a whole silent day would hardly smile or speak a few words. The answers may be just yes or no and with no eye to eye contact.
These are the patients’ characters that are deteriorated after the onset of the disease. For example, the asociality-where patient remains aloof, not interacting with anyone, avolition that is patient remain without any motivation for day to day activities or towards his job.
He may even sit whole silent day would hardly smile or speak a few words. The answers may be just yes or no and with no eye to eye contact.
Types of schizophrenia
-Depending upon the predominant symptoms patients are classified into
-Paranoid schizophrenia: where there are prominent delusions and hallucinations.
-Disorganized schizophrenia: where there are prominent disturbances in speech, behaviour and with no emotional responses.
Catatonic schizophrenia: here, the patient may have abnormal postures or gestures or movements like he may stand for hours at one place without any movement, or may wave his hands in the air continuously or repeatedly gesture like military salute at everyone or speak or repeat actions of others.
Residual schizophrenia: There are predominant negative symptoms or positive symptoms (the rest four) in a mild form.
Undifferentiated schizophrenia: where there is a complex cluster of all symptoms that don’t fit into any of the above four types.
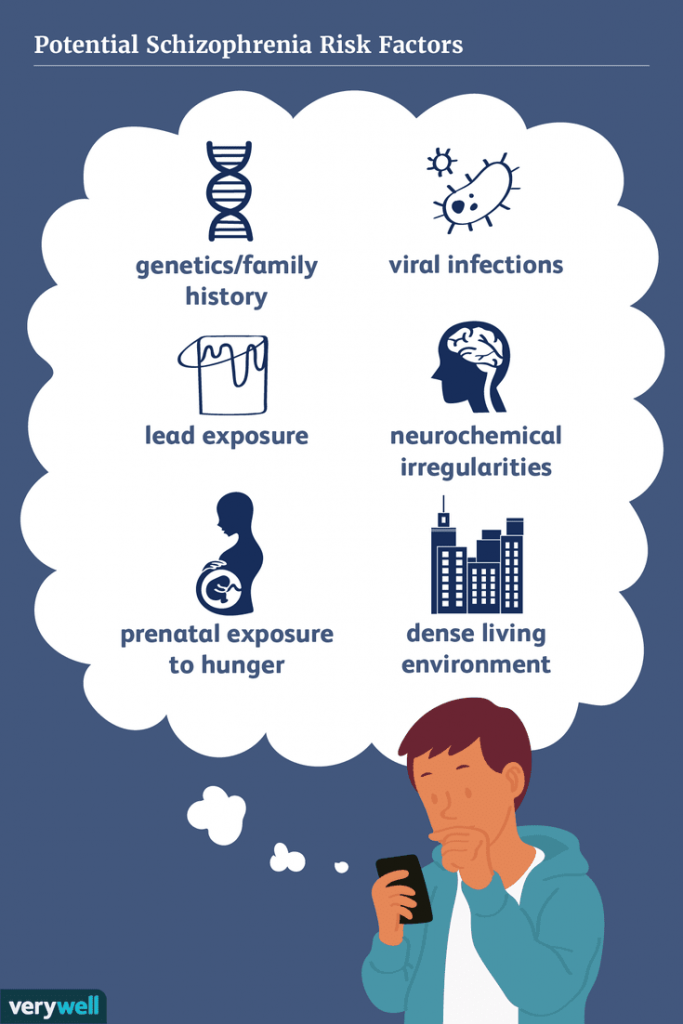
Causes of the disorder
There is no single pinpoint cause for the disorder, like in tuberculosis, caused by the bacteria named mycobacterium.
A combination of various entities causes schizophrenia right before birth, like abnormal genes, certain viral infection to the pregnant mother, difficult labour, childhood infections, abnormal parenting and abnormal personality etc.
Genes: Abnormal genes will cause unusual protein products and, thus, strange connections within the brain.
Birth complications: Prematurely, birth asphyxia, intrauterine viral infections.
These may cause an arrest or abnormal neural growth and connections. As the child grows into an adult, the symptoms start appearing.

Family as a cause for schizophrenia
Marital Skew
Describes the situation where one parent dominates the other.
Marital Schisms
Frequent conflicts between parents, where the statements are contradictory like the father said to do, and the mother tells not to.
Double Bind
Double binds occur when one person gives two mutually exclusive messages, e.g. when a child wants to eat ice cream, the mother, instead of saying yes or no, says “eat and get lost”.
Schizophrenogenic mother
A leading theory is proposing a possible psychological basis for the development of schizophrenia. This theory states that the mothers of schizophrenic individuals tend to be cold, rejecting, and yet controlling.
Pseudomutuality
This refers to relationships in which the family members appear to be civil and even friendly externally, but underneath the surface lies bitterness, resentment, and broken relationships.
Scapegoating
In certain families, scapegoat one individual for all the ongoing problems. This member carries the tag of a troublemaker and frequently scolded or rejected.
Extensive research now disapproves of the above theories as a causative role in schizophrenia, yet it is widely found in families with schizophrenic patients.
Life events(stressors), head injury, early use of cannabis may precipitate psychosis in a predisposed person.
Certain characters of the child, where it’s alone, lack appropriate emotional responses or no childhood friends(chums) or frequent tantrums and misbehaviours are usually found in future patients with schizophrenia.
Abnormalities in the neurotransmitters like Dopamine, Serotonin, Noradrenaline, Glutamate, GABA etc.,
Normal functioning of these chemical transmitters is required for thinking, feeling, and behaviour.
Expressed Emotions (EE)
These are the pattern of interactions and involvement by the caregivers of a mentally ill person, a high level of EE leads to an increased chance of relapse and poor prognosis of the disorder.
Low- Emotionally neutral acceptance, agrees with the patient, supportive and protective, engage in problem-solving discussion.
High- Critical, hostility, unrealistic expectations, over concern, judge patient behaviour negatively, attacks and counterattacks.

Diagnosis
A person is presenting with apparent symptoms of either two of the five symptoms running over the last six months and disturbing his occupation, family, and social surroundings.
These symptoms are not caused by any prolonged drug intake or due to a medical cause or a significant pathology in the brain (like a brain tumour).
Other associated symptoms:
Schizophrenia is commonly associated with
- Depression
- Excessive smoking
- Excessive water intake
- Suicide
- Other substances intake like alcohol, cannabis.
Management
Schizophrenia is treatable. Treatment with medicines and psychosocial support is adequate. However, most people with chronic schizophrenia lack access to treatment.
More than 69% of people with schizophrenia are not receiving appropriate care. Ninety per cent of people with untreated schizophrenia live in low- and middle- income countries. Lack of access to mental health services is an important issue. Furthermore, people with schizophrenia are less likely to seek care than the general population.
The management
-Schizophrenia is diagnosed mainly by clinical history taken both from the patient and the relatives, and other conditions are ruled out like drug intake. Appropriate investigations, like brain scans or tests for HIV, are done when required.
-Once diagnosed, the decision is made accordingly whether the patient requires an indoor treatment or management on an OPD basis.
-The level of insight, cooperatives, level of awareness among relatives, the facilities available, the severity of the disorder is all considered.
The methods available are
-Drugs – oral or injectable preparations
-ECT-Electro Convulsive Therapy
-Rehabilitation.
The Drugs
Drugs are classified according to their target of the action, broadly into
-Dopamine receptor blocker
-Dopamine and serotonin receptor blocker
Commonly used drugs (Dopamine blocker)
- Haloperidol 5-20mg
- Trifluprazine 5-20mg
- Chlorpromazine 50-100mg
These drugs are highly effective in acute stages but cause frequent side effects; hence usually not preferred for long term therapy.
The newer drugs (Serotonin-Dopamine blocker)
-Risperidone 2-8mg
-Olanzapine 5-20mg
-Quetiapine 50-600mg
-Clozapine 100-600mg
These drugs are now the first line of management yet have side effects like weight gain, sedation, orthostatic hypotension.
Clozapine is a novel drug preferably meant for resistant cases of schizophrenia, while it should be carefully used as it may cause agranulocytosis (0.1%), seizures (1-3%).
How long should it be continued?
-For acute symptoms, drugs are prescribed for at least one year.
-If the symptoms prolong for more than 1year, at least 3years, drugs to be taken.
-Most often, patients arrive late after two or three years, or when there are more than three episodes, lifelong treatment should be considered.
What are the precautions to be taken?
-Drugs should be taken according to the physician’s orders, and regular follow up is required.
-Medicines should not be stopped unless the treating psychiatrist said.
-When planning a pregnancy, the physician should be informed.
-Side effects should be reported at the earliest.
When ECT?
Electro Convulsive Therapy: it is indicated in most situations, like in acute cases, when the control of symptoms is required at the earliest.
-When the patient is in danger to him or his family, e.g., having suicidal or homicidal thoughts.
-When the patient is not having insight (awareness about the illness) and not taking drugs
-When a patient is not tolerant of drugs
-When there is associated depression or mania.
How safe is ECT?
-ECT is quite reliable, even when compared to drugs.
-There are only a few contraindications, like the presence of raised intracranial tension.
-The common side effects are headache, body ache, and temporary mild cognitive disturbances.
Rehabilitation
-Once the patient’s symptoms have reduced, the patient shall be referred to an occupational therapist and social organizations so that patients are taught to live a productive life.
-Rehabilitation is essential for recovery with vocational training. A person with schizophrenia will improve significantly with rehabilitation and become a useful member of the family and the community.
-Enhancing independent living skills through recovery-oriented psychosocial interventions (e.g. life skills training, social skills training) for people with schizophrenia and their families and caregivers; and
-Facilitating independent living, if possible, or assisted living, supported housing and supported employment for people with schizophrenia. This can act as a base for people with schizophrenia to achieve recovery goals. People affected by schizophrenia often face difficulty in obtaining or retaining regular employment or housing opportunities.
The course of the disorder
-Schizophrenia starts during late adolescence (17-27yrs) and continues with waxing and waning course over life.
-Only about 10% will have complete improvement, 40% will have a good outcome with occasional disturbances, another 40% will have mod-severe exacerbations often, and at least 10% have deteriorated.
Thus, early, active, and continuing treatment will have good outcomes in at least 60% of patients who can lead a productive life.